Article: Common Purpose: A model for enhancing complex service designs in the prevention of higher harm youth violence

Colm Walsh writes about Common Purpose, a public health implementation approach to tackling youth violence in Northern Ireland.
Introduction
A persistent problem
Violence is something of an enigma and responses to it are highly variable. The most recent global status report on violence against children (WHO, 2020) reports that 50% of children aged 2-17 experience some form of violence and more than one billion children and young people are exposed to interpersonal violence annually (Hillis, Mercy and Saul, 2017). Further, many children and young people do not experience violence as a single event, but as a condition of life (Falconer, Casale and Kuo, 2020). The effects of violence can be so enduring that preventing violence against children and young people is enshrined in the UN Sustainable Development Goals (SDGs) (e.g. SDG 16) and the UN Convention on the Rights of the Child (Article 19).
To achieve these standards and respond to national policy, a process of understanding complex needs at regional and local level is required. Public health approaches hold some utility. However, there are few accessible protocols of how these public health approaches are practically implemented – in other words, there are indicators of what could be implemented but little detail on how. This paper outlines a practically oriented public health approach using the ‘Common Purpose’ framework.
Complex responses to complex challenges
Given the complex issues facing communities, complex responses are often required. These responses vary greatly in terms of content, modality, duration, the population of interest, targets, costs and effectiveness. In the context of violence prevention, complexities can be exacerbated without coherent agreement on the problem, clarification on roles and responsibilities, and identification of contributing factors. To date, few frameworks have been considered that could help to facilitate decision making, design, implementation and evaluation (Abt, 2016). Whilst some comprehensive violence prevention frameworks exist (see for example Arnot and Mackie, 2019; Butchart et al., 2002), these do not concretely orient implementation teams towards practical solutions through the application of methodical decision taking and action making.
During 2019, a methodical process was undertaken in one community in Northern Ireland which became known as ‘Common Purpose’. This was supported by the Department for Justice in Northern Ireland and the actions were led by the Education Authority for Northern Ireland Youth Services, Police Service of Northern Ireland (PSNI) and local community groups. This framework has significant utility in addressing complex needs at local level through a structured framework for participants from diverse professional backgrounds and personal experiences to arrive at mutually agreed understandings of a contextually specific problem and identify goals. The remainder of this paper illustrates Common Purpose across three sections. (1) An overview of the approaches that helped to inform the practical steps of the Common Purpose framework. (2) An overview of the Northern Ireland case as an illustrative example where the steps involved in the methodical process are outlined. (3) The paper ends with a series of conclusions and recommendations for the refinement of the framework.
Northern Ireland context
Northern Ireland has a distinct context that has been dominated by pervasive inter and intra community violence stretching back to the 1970’s (Fay, Morrissey, and Smyth 1998). Despite the peace accord in 1998, the legacy of conflict has persisted. Violence remains a daily reality in some communities, with some young people at elevated risk of paramilitary threat, violence and exploitation (see for example, Harland, 2012, Walsh & Schubotz, 2019, Walsh 2019). The ‘Fresh Start’ Agreement, published by the UK and Irish governments in 2015, set out strategic proposals for addressing some of these challenging, and often intractable issues, becoming enshrined in the Northern Ireland Executive’s Programme for Government 2016-2021. Strategic priorities included:
- Promoting lawfulness
- Support for transition away from conflict
- Tackling criminality and criminal exploitation
- Addressing systemic issues undermining the transition towards peace
A ‘Tackling Paramilitarism’ project team and board was established that was tasked with working towards the attainment of these priority areas through a twin track approach: a combination of policing and justice efforts alongside activities to better understand socio-economic issues facing communities where paramilitaries are most active.
Escalation of public disorder
During 2018, there was increasing evidence of the criminal exploitation of young people by paramilitary groups in the city of Derry in the North West of Northern Ireland. This prompted a strategic review of coordinated youth services as violence increased exponentially during the Summer. Violence continued in the city and even escalated into 2019, culminating in the death of journalist Lyra McKee in April 2019. The necessity for a targeted, earlier intervention, community-based approach was reinforced and public health responses showed promise.
Public health approaches are widely accepted to be useful frameworks that aid the design and delivery of violence prevention efforts. The experiences in Glasgow and in Chicago are widely publicised and the public health approach has been identified by the World Health Organisation as one of the most favourable approaches in the prevention of injuries caused by interpersonal violence. A public health approach is anchored around monitoring complex issues through surveillance), identifying risk factors logically linked to the problem, designing and testing responses aimed at reducing the prevalence or impact of those same problems and then monitoring their effects.
Standard public health frameworks describe three levels of intervention: primary (universal), secondary (targeted) and tertiary (specialised) (Matjasko et al, 2012). Primary interventions often include weekly sessions, targeting a universal population under the age of 15, focus on strengths, and generally involve a shorter input (4-12 weeks). As risk increases, the nature of the input changes. Secondary approaches tend to focus more heavily on changing the natural environment (peer relations, family functioning, community relationships), are generally longer-term, and establish clear and measurable goals with young people (Manuel & Klint-Jorgenson, 2012). Tertiary responses are implemented by specialists to address acute pyscho-social concerns and can involve the application of evidence based therapeutic supports. Having a grounded understanding of the frequency, intensity and scale of violence being perpetrated will determine the type of intervention implemented.
However, what the public health literature often fails to do is provide a basis by which partners can practically implement a public health model. Further, the public health literature fails to help partners involved in the prevention of violence to connect evidence to need. In this example, the partnership developed a mechanism for doing this by extending the public health approach to include perspectives from both behavioural and implementation science and cutting edge violence prevention research.
A public health framework
Approaches informing the framework
Informed by a realist approach (Pawson and Tiley, 1997), the framework asks that users explore and identify the context that enable the implementation of activities and seek to understand the mechanisms that transform inputs into outputs and contribute towards the attainment of desired outcomes. Realist evaluations are theory incarnate (Westhorp et al, 2011) meaning that theory should emerge during the process. One of the tasks of realist evaluation is to make the theories within a programme explicit, by developing clear hypotheses about how, and for whom, programmes might ‘work’ by connecting practice wisdom to reliable empirical evidence.
As noted by Mihalic et al (2003) we already know a lot about what to implement but we are not quite as sure how to implement. Often overlooked, implementation approaches help participants to understand the interconnectedness between data, systems, delivery and culture (Durlak & DuPre, 2008). Without its application, interventions are less likely to reach those who most need them and activities are less likely to be sustained. This is evidenced by the fact that many ‘successful programmes’ are not routinely sustained over time (Rogers, 2003).
The process
Drawing on realist, implementation and public health approaches, participants were asked to consider key questions across four key domains: context; activities, implementation and impact (see table 1). The public health approach was drawn upon with reference to defining the problem, reviewing evidence for and against the problem, and identifying evidence-informed responses. Drawing on an implementation approach, participants are also asked to consider how activities are implemented, the systems that are in place to monitor and report on progress against desired outcomes, and the competencies of personnel required to undertake specific duties.
Table 1: Domain, questions and evidence
|
Domain |
Step |
Questions |
Evidence
|
|
|
|
|
RR=reflective review RCD-routinely collected data AD=administrative data MR=monitoring reports LR=Literature review |
| Context |
1 1 1 2
2
2 2
|
What are we doing and why are we doing it?
Where is the evidence of need? What does it say? What is the problem? What is driving and sustaining the problem across multiple systems? What are the most proximal drivers sustaining the problem? What outcomes are we trying to achieve? Are these feasible? Measurable? |
RR
RCD +AD
RR+AD +MR RR
RR
RR + RCD + AD +MR |
| Activity |
3 3 3 |
What activities have been implemented?
Which (if any) are directly linked to the problem? What does evidence say about their effectiveness in addressing the defined problem?
|
RR + RCD +MR
RR
LR |
| Implementation |
3
3 3 3 |
How are these implemented and by whom?
What are the roles and responsibilities within and between organisations? What systems are in place to monitor progress? How is data shared?
|
RR + MR
RR + RCD + AD
RR +MR
RR |
| Impact |
4
4 4 4 |
Which data links to the problem or desired outcomes?
How reliable are they? What do they show? What are the gaps?
|
RR
RR + LR RR RR |
Step 1: Alignment on need
Step one of the Common Purpose process requires significant time as this allows for greater and more sophisticated understanding of the context in which participants live and work and the range of issues that they experience (Pawson and Tiley, 1997). Participants are asked to identify the focal problem – the priority area that is the root of many other problems. These guiding questions are illustrated in table 1 and enable participants to reflect on the evidence of need and the rationale for undertaking (or intention to) specific work. In the Derry context, the most significant concern was increasing public awareness of community tensions and the escalation in violence. A second, related, element of this first step is to understand if evidence exists and the quality of that evidence. If insufficient evidence exists, this could require the active collection of focussed data. As one participant commented during the process:
All of our data was telling us the same thing. On the ground young people
were telling us about their experiences. With the availability of police data,
we could see increasing incidents of public disorder and violence. Evidence
from the community also suggested increased recruitment of young people
into paramilitaries.
As a result of step one, participants in this example defined the issue that they wanted to address as: ‘young people are victims and perpetrators of higher harm violence and disorder in the city of Derry’. Alignment between participants was an anchor that laid the foundation of developing purpose and the defining of an overarching goal. The ‘Common Purpose’ in this context was a desire to ‘ensure a safe city and the positive wellbeing of youth living in the city’. This was particularly relevant during 2019 and it was agreed that the exploitation of children and young people by paramilitary and organised criminal had to end. With this definition as the anchor, participants were able to overcome potential sensitivities and address competing priorities. One of the limitations in this example is that young people’s voices were absent from the process. Whilst they were represented by youth workers, and the data that was presented included qualitative information captured by those working directly with young people, including young people in these processes would add significant value.
Step 2: Alignment on what is driving the problem
Step two requires the facilitation of reflection around the nature of the problem by examining the factors that are most strongly contributing to it. The aim here is to review a complex issue to gain alignment on the central difficulty, whilst orienting participants towards what is possible to address through any subsequent intervention/s. Partners are asked to consider the problem across four systems – individual, family, society and services (Bronfenbrenner, 1979; Cirone, Bendix & An, 2020). Fig. 1 illustrates the outcome of that process.
Within the individual domain, the drivers, ‘low hope’, ‘lack of positive social supports’ and ‘not engaged’ emerged as priority areas. Actionable drivers included a lack of engagement with those most at risk, a lack of safe spaces, and a lack of targeted and coordinated positive youth development activities.
Within the family domain, two drivers emerged as priorities. These included, ‘low parental supervision’ and ‘limited family contact by services’. These were reduced to one priority, the need for increased family contact. This definition was important as participants made a distinction however between family support and family contact, with the former representing formal and often mandated supports, whilst the latter was considered a voluntary arrangement developed organically on the basis of mutual interest-the young person.
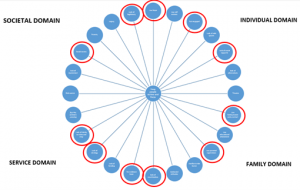
Figure 1: Drivers of the problem
The services domain included a perceived ‘lack of coordination’ between services, a limited ‘evidence base’ for activities, a ‘lack of strategy’ for the delivery of specialist youth interventions and a ‘lack of clarity on roles and responsibilities between participants’. Each of these drivers was reviewed and had one common drivers-lack of coherent and strategic partnership.
Finally, the participants considered the wider social domain and although several drivers were cited, the priority was the ‘social norms’ that continued to (at least tacitly) justify violence and the ongoing existence of paramilitary groups within the community. When this was reviewed a second time to examine what could be driving and sustaining this, it was found that attitudes continued to justify violence, there was work to do to enhance the perceived legitimacy of the police in some areas, young people had few positive alternatives to violence and community disorder and there was a lack of evidence base for these alternatives. From this review, a more focussed set of priorities emerged that (based on the data) was directly connected to the problem as it was defined.
Step 3: Reviewing the response
Step three requires participants to examine the activities that are implemented, how these relate to the problem identified in step 1, and links to the wider evidence base. All action, regardless of those responsible for its implementation, placed youth at the centre (Kia-Keating, 2011), a principle that anchored even divergent partners and help consolidate their commitment to the process. A large part of these required participants to focus on solutions rather than problems and in order to link solutions to need, there was a commitment to align actions with evidence. Routinely implemented activities included positive youth development activities that provided safe spaces for young people to test their values and beliefs, to engage children and young people in skills development work, to develop leadership capacity amongst young people and provide them with opportunities to take on leadership roles and to try and test new and innovative approaches. There was a recognition that many young people had been affected by traumatic events. For example, many of those engaged in community violence had been victims of violence themselves. The participants indicated that understanding the impact of trauma has helped to inform their practical response, particularly for those whose needs were more complex. As need increased, responses appeared to become more complex and specialised.
There was a decision to provide a responsive ‘Agile Response Fund’ provided the basis from which delivery partners could access the necessary resources in a timely manner. Whilst recognising the need for timely and responsive action, the participants also believed that activities needed to be planned and purposeful and directly connected to working towards the attainment of well-defined goals. The participants also drew upon a bespoke innovative model for ‘Steering Teenagers Away from Recurrent Trouble’ (START), a targeted outreach model with the aim of reducing the impact of paramilitarism and organised crime.
A review of these activities also illustrated ten principles that appeared to underpin all activity: 1. Youth centred; 2. Trauma aware; 3. Solution focused; 4. Committed partners; 5. Risk tolerant; 6. Accessible partners; 7. Planned and purposeful action; 8. Responsive delivery; 9. Evidence informed responses; 10. Innovative practice. Whilst these principles are somewhat unique to this context, understanding the principles that govern decisions and action consolidates alignment.
Step 4: Considering the impact
Ultimately, any targeted intervention seeks to have a tangible impact on the target population, as well across wider society. This framework connects steps one to three to enable partners to identify the areas that are more important to measuring, a space to review the data that is currently available and identify gaps that are require action. Connections in this example can be made between the priority areas being targeted, the anticipated outcomes and highly targeted measures that link them. Reviewing a range of routinely collected data as well as administrative data from the police, this review enabled participants to populate areas directly linked to the target areas.
By applying the Common Purpose framework to understand complex issues in this example, partners considered the context in which the problems were presenting, leading to alignment on a well-defined problem. This was supported by comprehensive review of administrative data, routinely collected data, and participant reflections. This coherent definition of a problem led to clearer identification of measurable goals and linked to these goals, roles were able to be attributed among participants making responsibilities clearer that they otherwise would have been. Combined, this process contributed to the development of a unique theory of change, specifically related to a particular context (see figure 2).

Figure 2: Theory of change
Conclusion
For many communities, violence is a reality of everyday life (Cuarta & Roy, 2012). The drivers are not well understood, and the responses are highly variable. At an international level, there are obligations to prevent violence against children and young people and at a strategic level, there are policy commitments that underpin delivery. However, to date, few frameworks have been described that help to facilitate such efforts. Taking the case of Derry, Northern Ireland, the ‘Common Purpose’ framework has significant utility to inform the coherent, methodical and evidence informed design of complex interventions. Central to the framework is the participatory and facilitative process that enhances alignment around sensitive issues, clarifies roles and responsibilities and tailored interventions, based on evidence, to needs. If it could be summarised more succinctly, the following formula might work:
Change is a function of assessed need (n) combined with alignment on the problem (p) including agreement of a set of common values (v) alongside mutually agreed interventions (i) and well-defined target areas (t).
This framework is designed for understanding complexity and responding to it in a focused but also localised way. By applying this framework, there is potential to focus partners’ minds on strategic, specific and measurable responses.
In future, replication of the model could ensure that the voices of young people are heard and that they are actively engaged in all steps of the process. This would provide additional insights into the complexities that contribute towards violence and criminal exploitation, enhance the value of the engagement process and increase the validity of the responses agreed.
Youth & Policy is run voluntarily on a non-profit basis. If you would like to support our work, you can donate any amount using the button below.
Last Updated: 19 April 2021
Acknowledgements:
Arlene Kee, Assistant Director of Youth Services, EANI; Stephen Quigley, EANI; Gordon MacCalmont, Superintendent PSNI; John Lynch, Long Tower Youth Centre
References:
Abt, T. (2016) Towards a framework for preventing community violence among youth. Psychology. Health and Medicine, 22
Arnot, J, and Mackie, P (2019) Violence Prevention Framework. Scotland: Scottish Public Health Network.
Bronfenbrenner, U. (1979) The Ecology of Human Development. Cambridge, MA: Harvard University Press
Butchart, A., Cerda, M., Villaveces, A. and Sminkey, L. (2002) Framework for interpersonal violence prevention: Framework development document. Geneva, Switzerland: World Health Organisation.
Cuarta, J. and Roy, A. (2019) The latent threat of community violence: Indirect exposure to local homicides and adolescents’ mental health in Colombia
Durlak, J.A. and DuPre, E.P (2008) Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation, American Journal of Community Psychology, 41(3–4), pp. 327-350
Hillis, S., Mercy, J., Saul, J. (2017) The enduring impact of violence against children. Psychology, health and medicine, 22(4), pp. 393-405
Kia-Keating, M., Dowdy, E., Morgan, M. L., & Noam, G. G. (2011). Protecting and Promoting: An Integrative Conceptual Model for Healthy Development of Adolescents. Journal of Adolescent Health, 48(3), pp. 220-228.
Manuel, C., Klint Jorgenson, A.M. (2012) Systematic review of youth crime prevention interventions. Copenhagen: SFI
Matjasko, J., Vivolo-Kantar, A., Massetti, G., Holland, K., Holt, M., Dela Cruz, J. (2012) A systematic meta-review of evaluations of youth violence prevention programs: Common and divergent findings from years of meta-analyses and systematic review. Aggression and Violent Behavior, 17, pp.540-552
Mihalic, S., Irwin, K., Fagan, A., Ballard, D. and Elliot, D. (2004) Successful program implementation: lessons from blueprints. Washington, DC: Office of Juvenile Justice and Delinquency Prevention.
Rogers, E. (1995). Diffusion of Innovations (3rd ed.). New York: The Free Press.
Walsh, C. (2019) Pathways and Outcomes: A review of what administrative data in NI can tell us about the prevalence and prevention of paramilitary and serious youth violence. Belfast, Northern Ireland: Department of Justice
Walsh, C. and Schubotz, D. (2020) Young men’s experiences of violence and crime in a society emerging from conflict. Journal of Youth Studies 23(5) DOI 10.1080/13676261.2019.1636012?journalCode=cjys20
WHO (2020) Global status report on preventing violence against children 2020. Geneva, Switzerland: World Health Organisation.
Biography:
Colm is a research fellow at Queens University Belfast with an applied academic interest in psychological trauma, youth violence, and evidence based practice and prevention.